

Abstract
Background:
TA-TMA is a life-threatening complication of hematopoietic cell transplantation (HCT), usually manifested as a combination of non-immune mediated hemolytic anemia, thrombocytopenia and end-organ dysfunction (renal, neurologic and/or hypertension). Reported mortality rates following TA-TMA are high (50-75%; Gavriilaki et al, Bone Marrow Transplantation 2017). It is more commonly associated with allogeneic HCT, however, may infrequently occur with autologous HCT. Traditionally, treatment for TA-TMA consisted in removing possible offending agents (calcineurin inhibitors, sirolimus) and/or instituting total plasma exchange (PLEX). These approaches have not resulted in significant improvement in the natural history of TA-TMA, with complete resolution in 12-20% of pts (Mulay et al, J Clin Apher 2015).
Recent evidence of alternate complement pathway activation has been implicated in the pathophysiology of TA-TMA (Jodele et al, Blood 2013). Eculizumab (ECU) is an anti-C5 monoclonal antibody, approved for treatment of PNH and aHUS, which has been used anecdotally as treatment for TA-TMA. Most reports consist of pediatric patients. In this analysis, we evaluated consecutive cases of adult recipients of HCT who developed TA-TMA and have received ECU therapy at our institution.
Methods:
We reviewed electronic records of consecutive patients who presented with a diagnosis of TA-TMA (non-immune hemolytic anemia plus worsening thrombocytopenia and end-organ dysfunction) and were treated with ECU between 2015 and 2017 at our institution. Univariate and bivariate statistics were calculated for the sample; Fisher's exact tests and Wilcoxon rank sum tests were utilized to test for differences across groups.
Results:
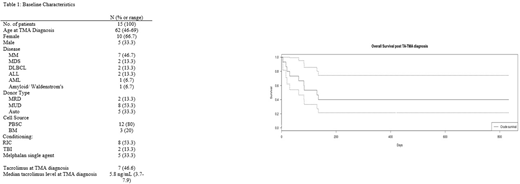
Table 1 shows the baseline characteristics of these pts. A total of 15 pts were included in the analysis; 2/3 were female and the median age was 62. ECU was given according to the usual schedule for aHUS (900 mg IV weekly x 4, 1200 mg every other week starting on week 5). Median time from TA-TMA diagnosis to initiation of ECU was 2 days. All patients received prophylaxis for Neisseria meningitides with ciprofloxacin and antifungal prophylaxis at initiation of ECU. Three (20%) pts received PLEX prior to ECU. Seven (47%) patients were receiving tacrolimus at diagnosis, however, levels were not within toxic range (3.7-7.9 ng/mL). Median time post-HCT for development of TA-TMA was 135 days. Median LDH, hemoglobin, platelet count and creatinine at TA-TMA diagnosis were 1724 U/L, 7.3 g/dL, 33,000/mcL and 1.7 mg/dL, respectively. Ten (66.6%) patients had acute kidney injury and 7 (46.6%) pts had neurologic manifestations. Eight (53.3%) pts had evidence of GVHD concurrent with TA-TMA diagnosis. Ten (63.3%) pts developed systemic infections during their TA-TMA treatment. No pts developed meningitis or fungal infections.
Median follow-up was 4.5 months after initiation of ECU. Eight (53.3%) patients had complete resolution of TA-TMA (i.e. resolution of hemolytic anemia, thrombocytopenia and end-organ damage), 4 of these 8 pts were recipients of autologous HCT. Median time to resolution was 98 days and median cumulative ECU dose was 10,200 mg (range 4800-36400mg). An additional 2 pts (13%) presented clinical improvement without complete resolution of TA-TMA.
Mortality secondary to TA-TMA or its complications was 33%. Median time to death was 31 days. The most common cause of mortality were infectious complications. Median survival for the entire cohort was 130 days (range 6-833 days, Figure).
LDH >1300 U/L; more than one organ involvement, allogeneic HCT, use of tacrolimus and early (<100 days) onset of TA-TMA post-HCT were associated with lower rates of TA-TMA resolution and higher mortality. PLEX prior to ECU did not correlate with improved outcomes.
Conclusion:
To our knowledge, this is the largest reported series of adult pts with TA-TMA who were treated with ECU. Treatment with ECU for TA-TMA is associated with higher rates of resolution and lower rates of cause-specific mortality than what has been previously reported with other approaches. We hypothesize that higher cumulative doses of ECU are warranted to achieve resolution of TA-TMA. A prospective study utilizing a more intensive schedule of ECU infusions is required to confirm such hypothesis. Based on our analysis, we conclude that ECU is an appropriate - and potentially better - option in the treatment of TA-TMA.
Skarbnik:Seattle Genetics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Jazz Pharmaceuticals: Honoraria, Speakers Bureau; Genentech: Honoraria, Speakers Bureau; Abbvie: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Pharmacyclics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Novartis: Honoraria, Speakers Bureau; Gilead Sciences: Honoraria, Speakers Bureau.

